








Between 10% and 20% of those who have lived through a traumatic event experience Post-Traumatic Stress Disorder (PTSD). Although commonly associated with combat veterans and first responders, PTSD affects millions of people across diverse populations.
But, compared to men, women are twice as likely to develop PTSD [1].
In terms of both symptoms and treatment outcomes, PTSD affects men and women differently, influenced by differences in types of trauma, biological factors, and coping styles.
Effective treatment for PTSD is best defined based on an understanding of these differences. This is not just in how symptoms present but also in how individuals respond to specific therapies and medications.
In this article, I highlight the importance of gender-sensitive care as I explore these issues
Different Symptoms and Comorbidities
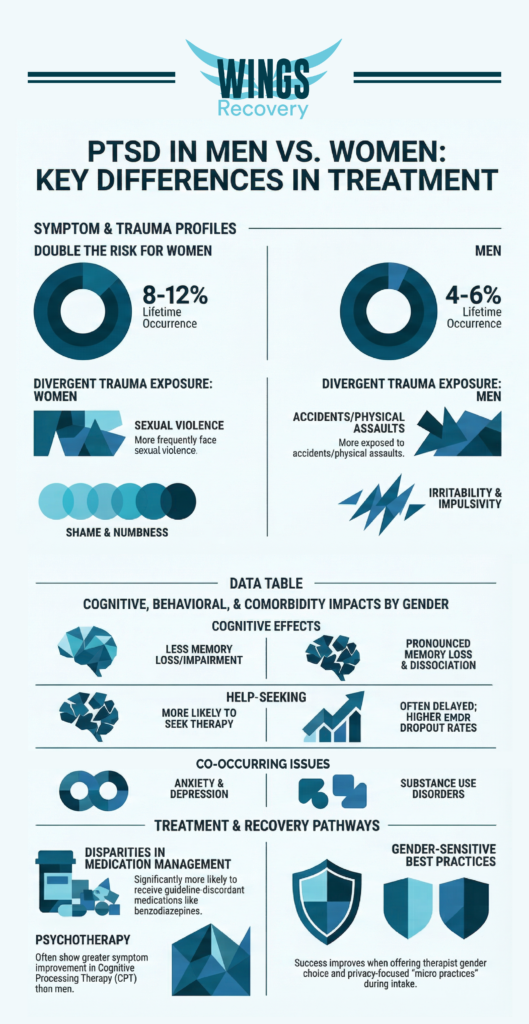
At roughly twice the rate of men, women develop PTSD, with a lifetime occurrence around 8-12% versus 4-6% in men. This gap reflects higher exposure by women to traumas such as sexual assault [1].
The type of trauma experienced often differs. Women are more frequently exposed to sexual violence. Men are exposed to accidents or physical assault. This should influence the focus of therapy.
Women tend to exhibit more internalizing symptoms, such as:
- Hyperarousal
- Emotional distress
- Emotional numbness
- Avoidance
- Anxiety
- Depression
- Shame
- Self-blame
- Intense re-experiencing of the trauma
- Higher rates of comorbid anxiety and depression
Men more commonly display externalizing symptoms, such as:
- Irritability
- Anger
- Impulsivity
- Paranoia
- Substance use
Men are also more likely to suffer from co-occurring substance abuse issues.
The key differences between women and men are summarized in this table.
| Aspect | Women | Men |
| Common Symptoms | Emotional numbness, avoidance, comorbid anxiety/depression | Irritability, impulsivity, substance use, and anger |
| Cognitive Effects | Less memory loss/cognitive impairment | More pronounced memory loss, hyperarousal |
| Key Differences | Women more often present with hyperarousal, intrusive re-experiencing, and interpersonal violence-related trauma. | Men commonly show dissociation and delayed help-seeking. |
Treatment Approaches
Evidence-based therapies such as Eye Movement Desensitization and Reprocessing (EMDR), among others, are proven helpful for both genders; however, there is still little research on this topic. A 2024 study of EMDR versus other therapies found no significant differences in PTSD symptom reduction, response rates, or remission between genders, but males had higher dropout rates from EMDR [2].
In general, men may need greater focus on anger management and substance abuse. Women may benefit from processing shame and working with women-only trauma-specific groups. Each may benefit from a supportive space in therapy to share experiences and foster healing from trauma.
Overall, women are prescribed more medications, possibly due to co-occurring mood disorders. And these include more benzodiazepines, despite guidelines against using them, due to the increased risks of dependency and adverse effects, particularly in women with trauma histories, which can complicate their recovery and therapeutic progress.
Response to Psychotherapy
A 2026 study on active-duty service members found that women with PTSD and major depressive disorder had a much bigger improvement in their symptoms with standard Cognitive Processing Therapy (CPT) than men [3].
The same study found that a combination of behavioral activation and cognitive processing therapy (CPT) made the differences in outcomes less clear. This suggests that men and women may need different types of therapy or different focuses.
Men are generally less likely to seek psychotherapeutic help than women, which can delay treatment and impact outcomes.
The Medication Puzzle
Veteran studies show that women are significantly more likely than men to be prescribed “guideline-discordant” medications—drugs like benzodiazepines or antipsychotics that are not recommended as first-line treatments for PTSD. [4]
While factors such as elevated rates of bipolar disorder in women explain part of this discrepancy, a substantial portion remains unexplained. This suggests potential gender bias or unrecognized symptom complexities in the presentation of women to clinicians.
Female-specific life stages (e.g., pregnancy, breastfeeding, meno
pause) and differences in drug behaviors complicate medication management and require a more tailored approach.
The Need for Gender-Sensitive Care
Women face a two- to threefold higher PTSD incidence than men. The setting and manner of care matter. In emergency departments and initial intake, women benefit from “micro practices” such as explicit consent before contact and privacy protection to prevent re-traumatization. These are elements of trauma-informed care best practices [5].
Clinical guidelines suggest offering patients a choice of therapist based on their trauma experience—for example, a preference for a specific gender—to improve engagement and safety.
While we know gender matters, research often fails to include diverse groups (like gender-minoritized individuals) or fully differentiate between biological “sex” and social “gender,” limiting the ability to tailor care for everyone [6] [7].
Key Takeaways
- Gender influences the effectiveness of therapy.
- Women are more likely to seek and respond to psychotherapy.
- Approaches that recognize this, such as male providers for men or female-led groups for women, improve engagement.
Gender-Specific Trauma-Informed Care in San Diego County
There’s no wrong time to get started with your journey of recovery. With our gender-specific treatment paths, our team understands your unique story and concerns. We believe in working with you so you’ll be an active participant in planning your journey alongside your dedicated medical team.
We don’t just focus on the specific aspects of your mental health. We address every area that needs improvement. This includes nutrition programs and other components of self-care. We see you for the person you are. You’re more than your mental health conditions, and your treatment reflects that.
If you want to know more about our programs at Wings Recovery, give us a call anytime at 760-359-9950.
Sources
[1] Fonkoue, I. T., Michopoulos, V., & Park, J. (2020). Sex differences in post-traumatic stress disorder risk: autonomic control and inflammation. Clinical autonomic research: official journal of the Clinical Autonomic Research Society, 30(5), 409–421
[2] Wright S., et al. nd. EMDR vs. Other Psychological Therapies for Posttraumatic Stress Disorder: A Systematic Review and Individual Participant Data Meta-analysis. Unpublished.
[3] Glassman L. et al. 2026. Sex differences in treatment outcomes among U.S. service members with comorbid PTSD and MDD. BMC Psychol. 2026 Jan 31;14(1):284
[4] Steffensmeier S., et al. 2024. What’s Gender Got to Do With It: Accounting for Differences in Incident Guideline Discordant Prescribing for PTSD Among Women and Men Veterans. J Clin Psychiatry. 85(2)2024 Jun 05.
[5] Larsen, S., et al. 2026. Mitigating Post-Traumatic Stress Disorder Risk Through Gender-Sensitive Trauma-Informed Care in the Emergency Department—A Narrative Review. The Journal of Emergency Medicine. Volume 80. 2026. Pages 241-251,
[6] Warren M, et al. 2026. Inclusion of sexual- and gender-minoritized individuals in randomized clinical trials of first-line treatments for posttraumatic stress disorder: A systematic literature review. J Trauma Stress. 2026 Jan 19.
[7] Langeland W and Off M. Sex and gender in psychotrauma research. Amsterdam UMC. European Journal of Psychotraumatology.

